Clinical Activities
-
User Trials with Spinal Cord Injured(SCI) Patients
-
 Under an NSF sponsored project (NSF 0649736), we conducted a study to explore the ability of individuals with SCI to use a WMRA (Wheelchair mounted robotic arm) to perform ADL (activity of daily living) tasks. The UCF-MANUS, a vision-based 6DOF assistive robotic arm, has been designed to aid individuals with arm function limitations to complete tasks of daily living that they would otherwise be unable to complete themselves. A small dual cohort pilot study with traumatic spinal cord injured (SCI) subjects was designed to investigate the utility of the UCF-MANUS for these subjects. Pick-and-place ADL tasks were defined and users trained and tested with the system for three weeks during which they controlled the robot either through a Manual or an Autonomous (supervised) mode of operation. Under an NSF sponsored project (NSF 0649736), we conducted a study to explore the ability of individuals with SCI to use a WMRA (Wheelchair mounted robotic arm) to perform ADL (activity of daily living) tasks. The UCF-MANUS, a vision-based 6DOF assistive robotic arm, has been designed to aid individuals with arm function limitations to complete tasks of daily living that they would otherwise be unable to complete themselves. A small dual cohort pilot study with traumatic spinal cord injured (SCI) subjects was designed to investigate the utility of the UCF-MANUS for these subjects. Pick-and-place ADL tasks were defined and users trained and tested with the system for three weeks during which they controlled the robot either through a Manual or an Autonomous (supervised) mode of operation.
Demographics
Ten individuals with SCI were chosen. Mean age of the subjects was 41.1(9.9) years and they were 16.7(11.8) years past date of SCI. All of their SCIs occurred from traumatic causes such as automobile crashes and falls. Initial diagnosis of subjects was between C3 and C7. Mean MMSE score was 27.7(1.64), and mean score on the self care subscale of the Functional Independence Measure (FIM) was 18.6(9.50). Additionally, MVPT-R score was measured to assess the user's visual perception independent of motor abilities - mean MVPT-R score was 57.2(5.01). Without the aid of the robotic assist device or help from other people, most of the subjects could not grab any of the six objects - only one subject was able to grab all the objects on the high shelf.
Inclusion/Exclusion Criteria
In collaboration with Orlando Health Rehabilitation Institute (OHRI - a part of Orlando Health), subjects were recruited from central Florida spinal cord support groups through advertisement and screened for appropriateness according to the following exclusion and inclusion criteria. Inclusion criteria are individuals who are 21 years of age or older and at least 90 days post traumatic injury and suffer from C3 to
C7 impairment. Candidates must be able to use a power wheelchair with joystick control (or other devices) as their primary means of mobility, and be cognitively able to perform tasks with a Mini Mental Status Exam (MMSE) score of 22 or greater. Additionally, participants must be willing to attend weekly videotaped training/testing sessions for a three-week consecutive time period. Duration of the weekly sessions will
vary between one and two hours. Subjects are to be excluded if they can independently perform self care activities of daily living (ADLs) as evidenced by a score of 40 or greater on the self care subscale of the FIM. Based upon an examination of medical records and test results conducted by clinicians at OHRI, qualifying subjects were asked to provide informed consent. Informed consent form was drawn from the research protocol approved by the Orlando Health and UCF institutional review boards.
Subject Grouping
Once enrolled, subjects were randomly divided into two cohorts to evaluate two control modes (Auto versus Cartesian) with the assistive robotic manipulator. Cartesian mode is where users command 3-D Cartesian position (forward, backward, left, right, up, and down) and 3-D orientation (yaw left, yaw right, pitch up, pitch down, roll clockwise, and roll counterclockwise) for the gripper at the end of the arm to enable interaction with the environment. On the other hand, Auto mode is where users click anywhere on the object of interest displayed on a screen as part of the scene captured by a gripper-mounted wide-angle video camera1. After the click, the robotic system transports and steers its end-effector to appropriately grab the object autonomously. Because of the use of computer vision based generation of motion, Auto mode users are not required to command multiple translation and orientation velocities at the end-effector. The subjects utilizing the Cartesian mode were classified as 'Cohort C' while the subjects utilizing the Auto mode were classified as 'Cohort A.'
 Experimental Setup Experimental Setup
A simulated ADL task setup was designed for user testing. Six ADL objects are placed on bi-level shelves and the user is asked to pick up each of the objects and bring them back to a specified spot. The different objects have varying shapes (curved and flat), sizes, and pose (upright versus laid down) - these objects were chosen based on top ADL items reported by clinicians in a survey conducted by us. The two shelves represent different levels of task, namely, easy and hard. We hypothesize that a task is considered easy when the object to be picked up is placed on a normal countertop level shelf (30" height) while it is categorized as hard when the object to be picked up is placed at the floor level shelf (6" height). Subjects' wheelchairs and items used in the ADL tasks were positioned in predetermined spots that were marked on the table and floor to ensure a consistent starting and stopping point for each task and for each user. The robot was positioned next to the subjects and not mounted on their wheelchairs due to the different hardware requirements of the various wheelchairs and the time it would take to mount the robot.
Outcome Measures
In the above setup, two quantitative performance metrics were employed. From the starting point to the stop point, a time to task completion (TTC) metric was stored to represent task completion efficiency while a number of clicks (NOC) metric was used for effectiveness of robot commands. When the user operated the robot, these two factors were automatically processed and saved in each user¡¯s database.
Study Protocol
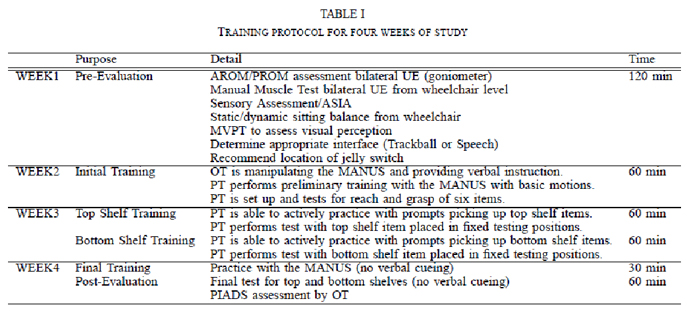
Prior to testing and training, all participants were given the opportunity to participate in a 90 minutes focus group. This focus group was utilized to study the ways that this group of participants train and learn. Study subjects were then evaluated by a therapist to ensure appropriateness and patient safety. Subjects were trained with the robot for one hour to two hours a day (depending on the week of the study), one day a week for three consecutive weeks. During week 1, an occupational therapist (OT) will directly assist the subjects to become familiar with both the MANUS and the interface, providing verbal feedback and physical assistance if necessary when performing different tasks with the robot. During the second and third weeks, subjects will practice using the robot independently but under direct supervision of an OT. A research assistant was in the same room for safety and in case subjects experience any technical difficulty with the equipment. Sessions were videotaped to allow for review as necessary. In the final week, PIADS assessment is administered by OT for qualitative analysis.
Data Analysis
Due to the small sample size, a nonparametric test was adopted to analyze the data. Wilcoxon signed-rank test was utilized to observe significant differences between the two cohorts using the TTC and NOC performance metrics. For testing the null hypothesis, alpha was set at 0.05.
Results
1. A Wilcoxon test examined the results of time to task completion (TTC) and number of clicks (NOC) of the given tasks with the WMRA throughout three weeks of study. First, our task discrimination into easy and hard levels seems appropriate in TTC; Z=-3.0854, p<0.05; and NOC; Z=-3.4327, p<0.05. Subjects completed easy tasks quicker and with less effort. Comparison between Auto and Cartesian control groups shows more interesting results. Overall performance shows a slightly significant difference in TTC; Z=-2.5135, p<0.05; but extremely huge difference in NOC; Z=-7.9615, p<0.05. It seems that Cartesian group caught up the speed of Auto group through three weeks of training. However, Auto group is superior to Cartesian group with definitely easy operations.
2. When we compared each weekly dataset with others, all subjects show a significant improvement in TTC; Z=-4.2664, p<0.05; and NOC; Z=-4.5576, p<0.05. Subjects completed the given tasks quicker and with less effort throughout three weeks of study. Transition from Week2 to Week3 outperforms transition from Week1 to Week2 in TTC; (W2W3) Z=-3.6636, p<0.05, (W1W2) Z=-1.568, p>0.05; and NOC; (W2W3) Z=-3.8078, p<0.05, (W1W2) Z=-1.7832, p>0.05. The more trained subject is, the more quick and easy subject completed the given tasks.
3. Within Auto group, easy and hard task categorization doesn't render any significant difference in TTC; Z=-1.4067, p>0.05; and NOC; Z=-0.0514, p>0.05. That is, Auto group was mainly affected by automated task execution but not affected by user's operation including panning and/or tilting of the robot's gripper. However, Cartesian group shows a significant difference in TTC; Z=-2.8275, p<0.05; and NOC; Z=-3.8366, p<0.05. In this case, hard tasks were more challenging than easy tasks because of time-consuming trajectory planning, occluded object with the robot's gripper, non-autonomous alignment of gripper with the target object, and non-autonomous closing of the gripper. For the easy tasks, Auto group shows similar performance in TTC; Z=-0.8065, p>0.05; but significantly easier in NOC; Z=-5.6463, p<0.05. This implies that three weeks of training helped a lot to improve the performance of Cartesian group in timing aspect. However, for the hard tasks, Auto group is superior to Cartesian group in TTC; Z=-2.6945, p<0.05; and NOC; Z=-5.6464, p<0.05.
4. Finally, we investigated learning effect in each group. Auto group shows steady performance in TTC; Z=-0.7714, p>0.05; but slightly improved performance in NOC; Z=-3.0904, p<0.05. That is, TTC is mainly ruled by the robot’s autonomous process but user's effort keep decreasing across training sessions. Of course, Cartesian group clearly revealed that subjects completed the tasks quicker in TTC; Z=-4.0828, p<0.05; and with less effort in NOC; Z=-3.684, p<0.05.
Reference
D.-J. Kim, R. Hazlett, H. Godfrey, G. Rucks, T. McNally, D. Portee, J. Bricout, and A. Behal, "On the Relationship between Autonomy, Performance, and Satisfaction: Lessons from a Three-Week User Study with post-SCI Patients using a Smart 6DOF Assistive Robotic Manipulator", 2010 IEEE International Conference on Robotics and Automation, May 3-8, 2010, Anchorage, AK, USA, under review.
-
Focus Group Meeting with Spinal Cord Injured(SCI) Patients
-
Under an NSF sponsored project (NSF 0649736), on April 21, 2009, a focus group was held at the Orlando Health Rehabilitation Institute to explore the process by which persons with Traumatic Spinal Cord Injury (TSCI) learn new assistive technologies (AT) designed to assist with activities of daily living (ADL).
The focus group was conducted as part of the Robotic Manipulator (MANUS) for Improved Independent Function study led by Principal Investigators Dr. Aman Behal of the NanoScience Technology Center and the College of Engineering at UCF, and Dr. David Portee of the Orlando Health Rehabilitation Institute. Dr. John Bricout of the UCF School of Social Work in the College of Health and Public Affairs (COHPA) joined this interdisciplinary effort as a research collaborator focused on integrating the social dimensions of the human-computer interaction in the MANUS project, beginning with a focus group aimed at exploring the learning heuristics of persons with TSCI. Preliminary focus group data informed exit survey questions targeting future MANUS design and implementation improvements, while the full analysis contained in this report will be used both to inform future training protocols, and to guide follow-up focus groups.
Reference
R. Hazelett, "Exploring learning heuristics for adopting new technology to assist with activities of daily living (ADL): Results of qualitative analysis using Nvivo 8 software", UCF/ARL Technical Report, July 2009.
-
Pilot Study with Multiple Sclerosis (MS) Patients
-
 Under an NMSS sponsored pilot project (PP 1069) that ended in June 2006, we conducted a study to explore the ability of individuals with MS to use a WMRA (Wheelchair mounted robotic arm) to perform ADL (activity of daily living) tasks. The WMRA used in this trial was the Raptor, which was developed by Phybotics, a division of Applied Resources Corporation, Wharton, NJ. The Raptor is a commercially available robot with four degrees of freedom. As explained in the following paragraphs, the results of this pilot study indicate that a WMRA is able to help individuals with MS with severe activity restrictions perform ADL tasks without the assistance of a caregiver and improve their social participation. Under an NMSS sponsored pilot project (PP 1069) that ended in June 2006, we conducted a study to explore the ability of individuals with MS to use a WMRA (Wheelchair mounted robotic arm) to perform ADL (activity of daily living) tasks. The WMRA used in this trial was the Raptor, which was developed by Phybotics, a division of Applied Resources Corporation, Wharton, NJ. The Raptor is a commercially available robot with four degrees of freedom. As explained in the following paragraphs, the results of this pilot study indicate that a WMRA is able to help individuals with MS with severe activity restrictions perform ADL tasks without the assistance of a caregiver and improve their social participation.
Demographics
Eight individuals with MS participated in the study. Mean age of the subjects was 55.3 years (8.7) and they resided in the long term care facility for a mean
of 5.1 years (4.5). Subjects were diagnosed with primary progressive, secondary progressive, or progressive relapsing MS.
Inclusion/Exclusion Criteria
Inclusion criteria included an EDSS score between 7.0 and 8.5, use of a power wheelchair with an upper extremity (UE) joy stick control as the primary means
of mobility, and a Mini Mental Status Exam (MMSE) score of 22 or greater. Subjects were excluded if they could independently perform self care ADLs as evidenced
by a score of 36 or greater on the self care subscale of the Functional Independence Measure (FIM).
Training
Prior to and after the a six week training period, it was shown that the subjects completed the five ADL tasks quicker and with less perceived
difficulty after the training. Without any training, subjects could perform the five ADL tasks more quickly without the WMRA than with it;
however, there was no difference in perceived level of difficulty in completing the tasks with or without the WMRA. After completion of the
six week training program, there was no difference between time to complete the tasks or perceived level of difficulty in completing the tasks
with or without the WMRA.
Results:
 1. At the end of the study, a greater percentage of subjects were able to complete each task with the WMRA than without it (see Figure 1).
1. At the end of the study, a greater percentage of subjects were able to complete each task with the WMRA than without it (see Figure 1).
2. Without the WMRA, three subjects could not complete any of the tasks and none of the subjects could complete all of the five ADL tasks.
3. With the WMRA, four subjects were able to complete all five ADL tasks, two subjects completed four of five tasks, and one subject completed three of five tasks, while only one of the eight subjects could not complete any of the tasks.
4. Visual Impairment was a big factor in that a strong inverse correlation was computed between:
(a) Total time to complete all five tasks with the WMRA and the subjects MVPT-R scores
(b) Self rated degree of difficulty when using the WMRA to complete tasks and the subjects MVPT-R.
| |
Spoon |
Cup |
Towel |
Cabinet |
TV
Remote |
| |
With
WMRAa |
Without
WMRA |
With
WMRA |
Without
WMRA |
With
WMRA |
Without
WMRA |
With
WMRA |
Without
WMRA |
With
WMRA |
Without
WMRA |
| S1 |
GDb |
CDc |
GD |
CD |
GD |
CD |
ModDd |
CD |
MinDe |
CD |
| S2 |
MinD |
NoDf |
MinD |
NoD |
NoD |
NoD |
ModD |
CD |
MinD |
CD |
| S3 |
GD |
MinD |
MinD |
MinD |
NoD |
NoD |
CD |
NoD |
MinD |
CD |
| S4 |
NoD |
CD |
NoD |
CD |
NoD |
CD |
MinD |
CD |
MinD |
CD |
| S5 |
MinD |
NoD |
MinD |
CD |
MinD |
NoD |
MinD |
NoD |
ModD |
CD |
| S6 |
GD |
CD |
CD |
CD |
MinD |
CD |
ModD |
CD |
GD |
CD |
| S7 |
ModD |
MinD |
CD |
NoD |
MinD |
MinD |
CD |
CD |
MinD |
CD |
| S8 |
CD |
NoD |
CD |
NoD |
CD |
CD |
CD |
CD |
CD |
CD |
| % Able to complete |
87.5% |
62.5% |
62.5% |
50% |
87.5% |
50% |
62.5% |
25% |
87.5% |
0% |
|
aWMRA=wheelchair mounted
robotic arm, bGD=complete task with great difficulty, cCD=cannot
do task, dModD=complete task with moderate difficulty, eMinD=complete
task with minimal difficulty, fNoD=complete task with no difficulty. [1]
|
Limitations:
| 1. |
Extensive insight into challenges with the
Raptor in particular and WMRAs in general was gained from data/video
analysis and patient feedback during our preliminary study. |
| 2. |
Data analysis suggested that: |
| |
(a) |
There was no difference in time to complete the tasks or
perceived level of difficulty with or without the device even after a long
period of training |
| |
(b) |
Untrained users were able to perform tasks faster without
the device than with it |
| |
(c) |
Visual impairment strongly correlated with increased time
to task completion and perceived degree of difficulty |
| 3. |
Patient feedback suggested |
| |
(a) |
Color coding the keypad controller with the corresponding
sections of the robotic arm |
| |
(b) |
Creating a key guard for the keypad |
| |
(c) |
Increasing the surface area of the gripper contact surface. |
| 4. |
Video analysis of the training and testing
suggested that: |
| |
(a) |
The four degrees of freedom on Raptor were not sufficient
as evidenced by inability to maintain orientation at the gripper while
ferrying back a grasped object |
| |
(b) |
Keypad may have been too small making it hard for users
with tremor |
| |
(c) |
Joint wise movement of the Raptor was not natural as
evidenced by user comments concerning their needing to concentrate a lot
to bring about right combination of movements |
| |
(d) |
Left and right designation on the keypad for the motion of
a joint was inverted after its preceding joint went through a large angle
of rotation. |
Reference
G.D. Fulk, M.J. Frick, A. Behal, and M. Ludwig, "A Wheelchair Mounted Robotic Arm for Individuals with Multiple Sclerosis: A Pilot Study", presented at the Combined Sections Meeting of the American Physical Therapy Association , Las Vegas, NV, February 9-12, 2009, abstract available in vol. 32, no. 4, Journal of Neurologic Physical Therapy, Dec 2008.
-
Questionnaire for Semi-Structured Exit Interview
1. In general, how would you characterize your exposure to using computers, either for use at home, school, or work?
2. In general, how would you characterize your exposure to using game consoles or computers for the purpose of entertainment?
3. How comfortable are you using computers?
4. What features of the robot itself and/or robot's interface did you find most useful?
5. What features of the interface did you find less useful?
6. Concerning the less useful features, how would you recommend we change these to make this a better device?
7. Are there any additional features/options that you would recommend adding to the interface?
8. Are there any changes that you would like to see made to the robot arm itself?
9. Which was more difficult - directing the robot arm close to the object or getting the robot arm to grab the object once you got close to the object?
10. Were you provided enough time to learn the system?
11. Did you get a chance to use the robot in both the modes during the course of the study? If yes, can you compare the advantages and disadvantages of both the modes?
12. What are some other tasks that you are interested in performing with this system, but the robot was not able to assist you with?
13. Are you able to pick up and grasp things easily on your own?
14. What are some of the specific tasks that you think this device could be most useful for?
15. Would you be interested in buying this device, if money were not a factor?
16. In its current state, do you feel that the robot would make you more independent and improve your quality of life? If not how would you modify the robot so that you could be more independent with it?
17. If you needed help with the MANUS do you feel that you could explain its operation to others?
18. Have you talked to other patients in this study about what you have learned about the MANUS?
|
|
|